I made a little movie to help make it clear.
|
The CDC used to publish what they referred to as a surveillance of hysterectomy in the U.S. every 5 or so years. Since 2005, they've stopped, or at least stopped publishing them online, and have even taken down the 2000-2004 report.
Apart from surveys that are done only very infrequently, the last one being in 1996, the CDC has only ever published the number of inpatient hysterectomies. This is the basis for the number we see cited so commonly in studies and literature, 600,000. However, this is increasingly inaccurate as the level of outpatient, or ambulatory, hysterectomies rises. A well-corroborated number from the AHRQ indicates that at least 40%-50% of all hysterectomies are now done on an outpatient basis. This doesn't mean that the patient goes home the same day. An outpatient patient can actually end up spending several nights in the hospital but the doctor never admits her. Her insurance likes this because they pay less for an outpatient procedure. Anyhow, if we use the 40% figure, we know that the last-reported CDC inpatient number was 498,000. That means that, if inpatient is 60%, that's about a 830,000 total of U.S. hysterectomies. To arrive at the number of elective hysterectomies, let's be really conservative and take out every woman diagnosed with uterine (55,000), ovarian (22,000), and cervical (13,000) cancer, based on SEER stats (e.g., http://seer.cancer.gov/statfacts/html/cervix.html). That leaves 740,000 elective (voluntary) hysterectomies. If we stick with the accepted "55% of elective hysterectomies include bilateral ovary removals" estimate, that's about 407,000 women a year whose ovaries are removed during elective hysterectomy. However, the number of healthy ovary removals may increase to ~700,000 a year if Dr. Rocca is right in his write-up that there are 300,000 additional BSOs when women present with benign cysts. Potentially, we are talking about ~1,900 women a day to remove an organ that only develops cancer in 22,000 women a year. But are all these random ovary removals the reason the number is so low? No. The ovarian cancer diagnosis and mortality rate was the same in 1965 when the ovarian removal rate was only 25%. With such a low risk, removing the ovaries of a woman at risk is like shooting fish in a barrel. Taking out hundreds of thousands to address the risk in ~20,000 is like using a boulder to crush an ant. It's also not a surgical approach taken in any other cancer prevention surgery. The ACOG argues that this should ultimately be up to the woman. Unless the woman does not have a demonstrated (via a certified genetic counselor) risk of ovarian cancer, this is not true. Once the doctor says "cancer risk" to the patient, she will agree to anything. If they couple that with their 2011 brochure that says that the ovaries cease functioning at the time of menopause, which we've known for 100 years since the endocrine system because well-understood is not true, then you are setting up enough misinformation for us to stay where we are: hundreds of thousands of women made ill to address a microscopic risk. This is NOT about informed consent, but about bad medicine. The statistics are staggering. Why women without ovaries are more likely to develop Alzheimer's and other dementia; Parkinson's; and lung cancer - a hypothesis. Also, why calcium supplements are not the answer to our increased risk of death by fracture.
 Researchers increasingly tie high LDL (low density lipid, a.k.a., bad) cholesterol to the Lewy bodies/plaque that they see in these patients. They see the high cholesterol affect patients who've had some kind of heart or TBI (traumatic brain injury) issue, but I'd guess that not being able to regenerate normally because activin is absent could have the same result. Without a response from the ovaries to the luteinizing hormone (LH) sent to them by the pituitary gland, the luteinizing hormone levels just keep going up, unchecked. Higher levels of luteinizing hormone are also tied to Alzheimer's in women, so the risk profile of women without ovaries becomes more complex but the fact that she has increased risk becomes clearer. (LH/Alzheimer's study here: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2111407/ - though the study author is incorrect, of course, when she says that postmenopausal women have lost their ability to produce estrogen. This is not true of either BSO women or naturally postmenopausal women, but is more true of BSO women. At a minimum, the adrenal glands contribute androgens that convert to estrogen. In women who keep their ovaries, their testosterone rises after menopause and some of it converts to estrogen, leading to higher levels in postmenopausal women than BSO women.)  My thinking is that it is the missing activin, a cytokine protein produced by the gonads (ovaries), at play when there are issues with the lungs (also the arteries, due to activin's role in elasticity and smooth muscle). Lung alveoli rely on activin. This may be why I read about (and have personally experienced) asthma as one of the first health issues in BSO women, and may also be the reason that regeneration issues and lack of activin (cytokine) activity to reduce inflammation lead to lung cancer and other lung issues, even in women who haven't smoked. We know that using hormones, as many women without ovaries do, increases this risk even further, to 2.4x. 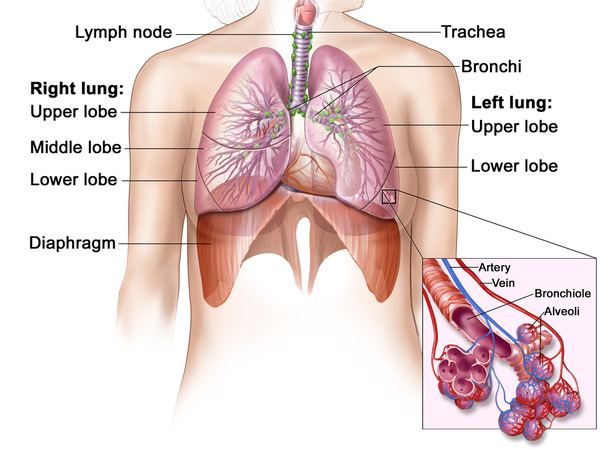 The significantly lower testosterone they find in women without ovaries, in, for example, the Fogle and Rancho Bernardo studies, is one aspect of heart and other muscular weakness, but activin is likely a separate contributory factor.
Finally, this week's article in the New England Journal of Medicine about the fact that calcium supplements weren't show to reduce fracture is not surprising. Fracture is not so much about bone mineral strength but about bone's flexibility that comes from the net made by collagen. The lack of flexibility that comes with the decline in collagen in bone is likely the underlying issue with fracture in women without ovaries, not the lack of calcium in her diet. Our bones are more brittle for the same reason that our skin is dry and lifeless. It's also the reason so many of us experience painful osteoarthritis and fibromyalgia - lack of collagen in joints. Activin is too often overlooked, and contributes to a host of health issues of its own. I keep coming back to it as our biggest blind spot with women who've had a BSO. Alzheimer's costs the U.S. $2 billion a year right now, and that number is projected to increase 5x by 2050. Maybe we could check some of that if we stopped removing healthy ovaries 1,900 times a day in this country. For more information, visit www.overy.org or email at [email protected]. Today, I just write to link to this Philly Inquirer op-ed by Dr. Hooman Noorchashm, a cardio-thoracic surgeon, who writes about the issues with inadequate surgical training of OBGYNs.
Link to it here: Gynecological surgery: Second rate training for second rate patients? If we were to look at scale, given the female population in the U.S. now, a snapshot of numbers, though surgery continues on a rolling basis, could look like this (I promise this is very simple math): There are ~160M women in the U.S. today. 40% will have a hysterectomy. That's 64,000,000 hysterectomies when those women are between 45-54 (source: Dept. HHS) 55%, or 35,200,000 women, of those women's ovaries would be removed during that hysterectomy. And that number almost doubles if the women whose ovaries were removed during surgery for benign ovarian cysts are added in...but let's play it safe and say that: 50 million women who are alive in the U.S. at this moment, women who have absolutely nothing wrong with their ovaries that requires removal, could end up having a surgery described this way. How much would those surgeries bring in at today's rate of $33,180 per surgery average (source: AHRQ)? $1,659,000,000,000 - that's 1 trillion, 659 billion dollars...just for elective ovary removals folded into hysterectomy/cystectomy elective surgeries. What was the thinking about this surgery at the end of the 19th century?  This question has been, for many women, part of the underlying issue in the debate about women's health and legislation. How possible is it for a majority of men to justly legislate an issue that can never affect them personally? This same question makes sense when applied to the guidance and opinions that come from the ACOG. Of the 65 past ACOG presidents (they change annually), there have been 40% more named Richard than women in entirety. The ACOG's attitude toward the issue of morcellation is well-documented. Their attitude toward removing women's healthy endocrine glands is no different.
As I've been working with doctors in the UK who will be doing a systematic review of all of the studies related to increased disease risk that result from removing the ovaries, they let me know that 8,795 studies that might be related to this surgery have turned up in a Cochrane Library search. My first thought was, "Wow, that's a lot..." My second thought was, "What a devastation. This is science...all curiosity, no conscience." Would this devastation have happened to men in our wildest dreams? At what point was it going to occur to physicians and researchers that this was a sinister modality - harm women, then study the effects? We've seen this before in history, but never on this scale. Would it have gone on forever? Will it if I am unsuccessful? Every day, another 1,000 women are made ill when their HPG axis is dismantled and their endocrine circuit board is short-circuited. These women may not participate in studies, but their surgery took place despite what studies have told us for 100 years. The knowledge that this continues unchecked is crushing. Premature death, Parkinson’s, Alzheimer’s, dementia, cognitive impairment, memory impairment, osteoporosis/fracture, cardiovascular disease, stroke, arteriosclerosis, sexual dysfunction, lung cancer, type II diabetes and metabolic disorder, depression, glaucoma... We at OB/GYN Reform are demanding a Congressional investigation into the decades-long practice of removing healthy ovaries in women without proven increased risk of breast or ovarian cancer. We believe the government's failure to regulate a multi-billion dollar industry has left room for that industry's judgment to spiral out of control, resulting in serious health crises in women of an age, where health issues are not considered or addressed, who have become a profit center for this specialty. The 740,000 annual elective hysterectomies 242-244 in this country (those not to treat diagnosed cancer, source: AHRQ & CDC) cost an average of $33,130 per surgery according to the AHRQ. That's $24,516,200,000 a year.
Can 40% of a 160 million person population (source: HHS) truly require an elective major surgery? Why is no one asking this question? Why does removal of healthy ovaries matter? Because, despite the fact that only 2% of all women are able to be diagnosed with a genetic predisposition to breast or ovarian cancer and might benefit from this surgery, the OB/GYN medical specialty removes the ovaries at time of hysterectomy for benign conditions like fibroids or endometriosis a staggering 55% of the time. (This percentage may be higher, but the CDC stopped publishing this data in 2000. We know it is very unlikely to be lower because it has risen from 25% in 1965 to 40% in 1984 to 55% in 1999.) It is also done in an additional 300,000 women who have benign ovarian cysts, which brings the number to at least 700,000 women a year. In fact, this year, scientists finally began to ask how helpful this surgery has been in the reduction of BRCA 1/2 breast cancer. The answer? It has not been. (Read more here.) The ovaries are not, as commonly believed outside of medicine, part of a hysterectomy. Hysterectomy only includes the uterus, and possibly, cervix. The ovaries are part of both the exocrine (ducted, in this case, egg-producing) and the endocrine systems. It's proven that their endocrine function does not stop working at menopause, and many studies published in the American Congress of Obstetricians & Gynecologists' own medical journal detail the fact that this surgery leads to significantly increased risk of significantly premature mortality resulting from diseases including up to 7x risk of heart disease, 2x lung cancer, fracture due to severe osteoporosis, Alzheimer's and other forms of dementia, Parkinson's, and many more. Removing the ovaries does not result in "early menopause"; it results in sick women who die prematurely. The practice makes no sense and must stop immediately. Under Section 1557 of the Affordable Care Act, women should be protected from disparate treatment in hospitals, the majority of which receive federal funding. Ovaries and testes are both gonads. They have homologous functions in the body's HPG axis. 1,000 healthy sets of ovaries are removed each day "to prevent cancer." Removing testes is the "gold standard" in preventing prostate cancer, which kills twice as many men each year as ovarian cancer kills women. How many preventative testis removals take place each day? Each year? It's never done. Though the mortality rate is double, the surgery is never performed in men without diagnosed cancer who've tried hormone suppressant treatment first. We must thank Senator Mark Warner, who wrote on Aug. 6 to say, "Thank you for contacting me regarding issues with the professional judgment of OB/GYN doctors. I've taken the liberty of contacting the Food and Drug Administration on your behalf asking that they review your concerns and get back to me with a detailed and appropriate response. As soon as I receive a reply, I will again be in touch with you. To sign up for my newsletter please visit www.warner.senate.gov. Sincerely, MARK R. WARNER United States Senator" However, we wrote to the FDA also, and they don't think they're the right agency since the issue is unrelated to pharmaceuticals and devices. We must also thank Virginia Governor Terry McAuliffe for sending the issue to the Virginia health department for a response on August 28, and Congressman Gerry Connolly for writing to Dr. Nancy Lee, head of Women's Health within the Department of Health & Human Services on September 1, 2015. These are important steps, but the most important is a Congressional hearing. Why? Because there is no possibility that any health advisory group can come back with the opinion that disassembling healthy endocrine systems is ever ok. Because there is no question that the removal of healthy ovaries, which is done a staggering 1,900 times a day, is harmful. The OBGYN specialty has things to answer for. We need access to a forum to share the harm these surgeries have done to millions of women, and to put an end to these types of surgery once and for all. www.gynreform.com Hysterectomy has been done vaginally since 120 A.D., and through a laparotomy, as with a c-section, since the mid 1800s, centuries before the advent of the morcellator. 92% of hysterectomies are elective surgeries for benign conditions: fibroids, heavy bleeding, endometriosis. Though these conditions are painful without question, none represent conditions we'd risk upstaging cancer to an incurable level for - agreed? As far as the way the surgery is performed goes, there are no circumstances under which a morcellator, a stick blender-like device used to chop up the uterus so it fits out the holes of a laparoscopic surgery, is required. More women agree to surgery when it is referred to as "minimally-invasive," sure, but the question is whether they would agree to this if they knew it increased their risk of death. An even better question is why doctors would propose it, given how obvious it is that grinding up potential cancer inside the body can never be preferable to removing it intact. Yet, that's what's been done for a couple of decades now, and that's what continues, even after the well-covered case of Dr. Amy Reed, brought to light through her tireless advocacy and that of her husband, Dr. Hooman Noorchashm, as she fights her upstaged cancer and they continue to work and to raise their 6 children. Because they pressed the issue, the FDA reworked the ACOG's math. The ACOG had been saying that the risk of a fibroid turning out to be cancer was 1 in 10,000. In fact, the FDA concluded, the risk is 1 in 352. The ACOG hadn't been using the right denominator to arrive at the risk. They'd been using "all women in the U.S." versus "all women who presented for surgery with fibroids." Even according to the ACOG's own guidelines for when to perform a hysterectomy, this surgery is performed far too often. Other types of surgeons, those who are trained in general surgery (OBGYNs are not), remove illness, not entire organs. In the cases where women's fibroids turned out instead to have been sarcoma (cancer), had the cancer been removed in place ("in situ"), it certainly would not have been upstaged in the manner in which it is when a morcellator is used. As you're reading these notes, which are directly quoted from the ACOG's May 2015 Annual Meeting, it's helpful to be aware that Dr. Keith Isaacson was a member of the panel that heard women's testimony to the FDA in 2014 about the fact that the women's cancer had been rendered incurable through the use of morcellation. Dr. Isaacson was allowed to remain on the panel despite the fact that he had a known financial conflict, having received money from robotic surgery device makers. You can read about that here. The original ACOG meeting notes can be found here. Directly quoted from the ACOG's May 2015 Annual meeting: "Mathers Lecture to Focus on Power Morcellation Concerns Posted By: ACOG on: May 03, 2015 This year’s John and Marney Mathers Lecture will consider the risks and rewards of power morcellation. “Morcellation Debate,” coming on the heels of last year’s FDA safety communication about the procedure, takes place at 3:15 pm today in Hall D and features Keith B. Isaacson, director of minimally invasive gynecologic surgery and infertility and Newton-Wellesley Hospital in Boston, and Javier F. Magrina, MD, professor of obstetrics-gynecology at the Mayo Clinic in Arizona. They will debate power morcellation’s benefits, concerns, sequelae, prevention of complications and the use of alternate techniques. The communication, first released in April 2014 and updated in November, warned against using laparoscopic power morcellators in most patients undergoing hysterectomy or myomectomy for uterine fibroids because of a risk of spreading unsuspected cancerous tissue, notably uterine sarcomas, outside the uterus. Contraindications include suspicion of cancer, menopause and small uterus. The risk of sarcoma in a fibroid exists, and morcellation of that fibroid may spread and upstage the disease, Dr. Isaacson said, but the treatment decision should rest with the patient and her health-care provider. “We just don’t have enough additional information to say that this is considered bad medicine because there are many advantages to a smaller incision, depending upon the patient’s preferences and her lifestyle and priorities, she may elect to do that,” said Dr. Isaacson, who was on the FDA panel that looked into power morcellation but didn’t work on the final document. The FDA document lists several contraindications. But for many younger or perimenopausal women, the procedure has great benefits that must be considered. The FDA and physician statements from ACOG, the AAGL and other organizations that have examined existing data still provide an opportunity for the informed patient to make the final call. “I don’t care what number you pick. Let’s say the risk of cancer is 1 in 10 instead of 1 in 8,000,” he said. “I still think the patient should be involved in the decision-making process after a discussion of the benefits vs. the risks.” Dr. Magrina opposes any morcellation that takes place outside an endobag. He will argue that morcellation safety will improve with use of endobags to contain the morcellated material. “Stopping only power morcellation doesn’t stop the problems that happen with morcellation by other means, such as using a regular cold knife if what you’re morcellating is exposed to the intraperitoneal cavity,” he said. Dr. Magrina said that the FDA missed an opportunity in its safety communication by not addressing the use of endobags. More companies are working with contained morcellation concepts that will improve patient safety. “I’m actually con and pro depending on how you do it — contained or uncontained,” he said. “The point that I’m making has never been discussed at the FDA level.” While concerns about spreading and upstaging cancer have grabbed most of the attention, Dr. Magrina said that more people develop benign conditions such as endometriosis and peritoneal leiomyomatosis that spread into the peritoneal cavity during morcellation done without an endobag. “The problem is not only with cancer,” he said. “And it makes no difference whether the morcellation is by knife or power morcellator.” In this 2014 video, you can hear the doctors explain that they would all perform morcellation. "The current situation with morcellation has not changed my practice in any way." So, what are these OBGYNs saying about endobags to contain the pieces and what are they saying about screening beforehand? Dr. Reed was carefully screened before her surgery. Any use of an endobag is an experiment at the patient's own risk, designed only to allow OBGYNs to keep using unsafe devices. According to the ACOG's own May 2014 Morcellation special report, endobags can tear or block the surgeons view: "Use of a Bag During Morcellation in Gynecologic SurgerySome investigators have suggested that the use of an intra-peritoneal bag during manual or power morcellation may be helpful in reducing intraperitoneal tissue dissemination (8, 30). However, power morcellation performed within a bag is not well studied and has several limitations that potentially increase the risk of the procedure. For example, currently available bags were not designed specifically for use in conjunction with power morcellation. The bags often have size limitations and have not been adequately constructed to prevent tearing by the morcellator. Further, the use of bags limits simultaneous visualization of the tissue being morcellated and the surrounding tissue that must be protected from the sharp morcellator blade." The third doctor in the video says that if a patient is at "low risk" of cancer, he would "absolutely" use a morcellator. Is that good enough for you? In Boston, hospitals disagree as to policy. Now imagine if, instead of figuring out better ways of dealing with uterine sarcoma, surgeons were sitting around constructing studies about how much it would cost not in lives, but in money, not to keep doing it? At Northwestern, that's exactly what they did. Is that how you imagine residents and surgeons spending their time? "Conclusions: Eliminating morcellation hysterectomy as a treatment for myomas is not cost-effective under a wide variety of probability and cost assumptions. Performing laparotomy for all patients who might otherwise be candidates for morcellation hysterectomy is a costly policy from a societal perspective." This isn't the first study of its kind, either. The device manufacturer, Ethicon, sponsored this one in 2011 before the doctors broke their story. Some OBGYN device advocates think it's ok to argue that we can't let go of technology. Though hospitals have invested heavily in these robots, that's not an excuse to keep using them if they're unsafe. In terms of policy, who makes policy if not the FDA? Their conclusion was to put a warning on the device, but they chose not to ban it. What about the ACOG? The ACOG's advice to its 58,000 OBGYN members was to continue to use the device, but, as usual, to put the onus back on patients. Their Committee Opinion in May 2014 was to inform patients of risk and to create a national registry of women made ill by the device. Does that make sense to you, as a patient? Once a physician suggests performing a surgery a certain way, doesn't that bias a patient even if only by making the patient consider that option? Would a patient imagine that something being offered could take something bad and make it worse? So, again, Dr. Keith Isaacson from Newton-Wellesley Hospital, who "doesn't care if 1 in 10 fibroids is sarcoma," is in favor of morcellation. As with study results, it's important to follow the money:  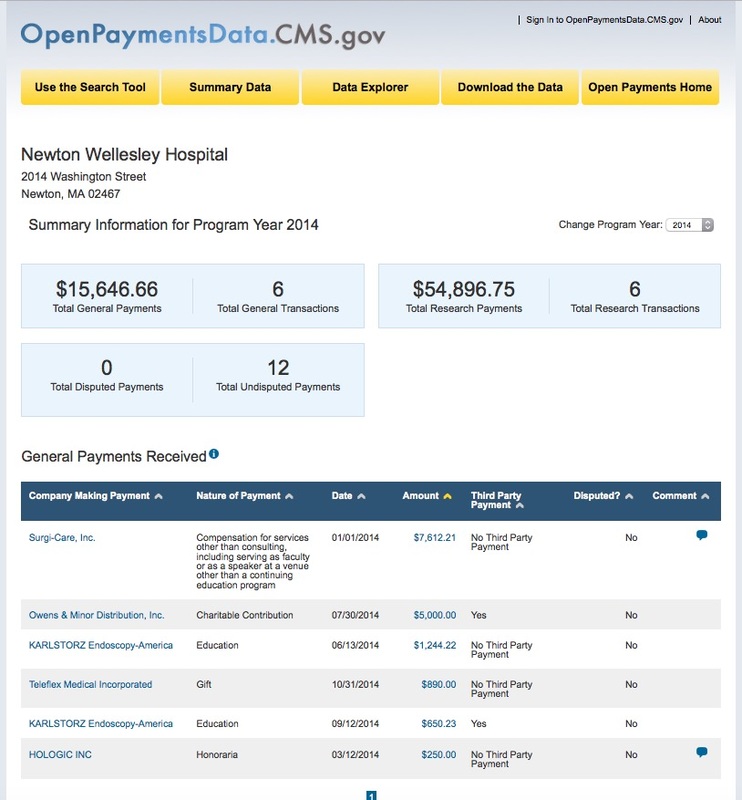 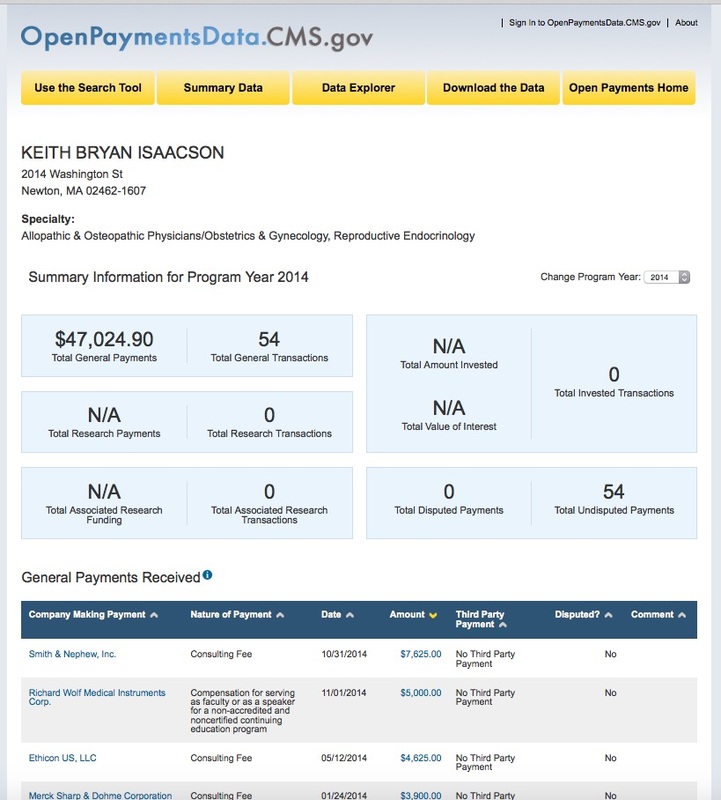 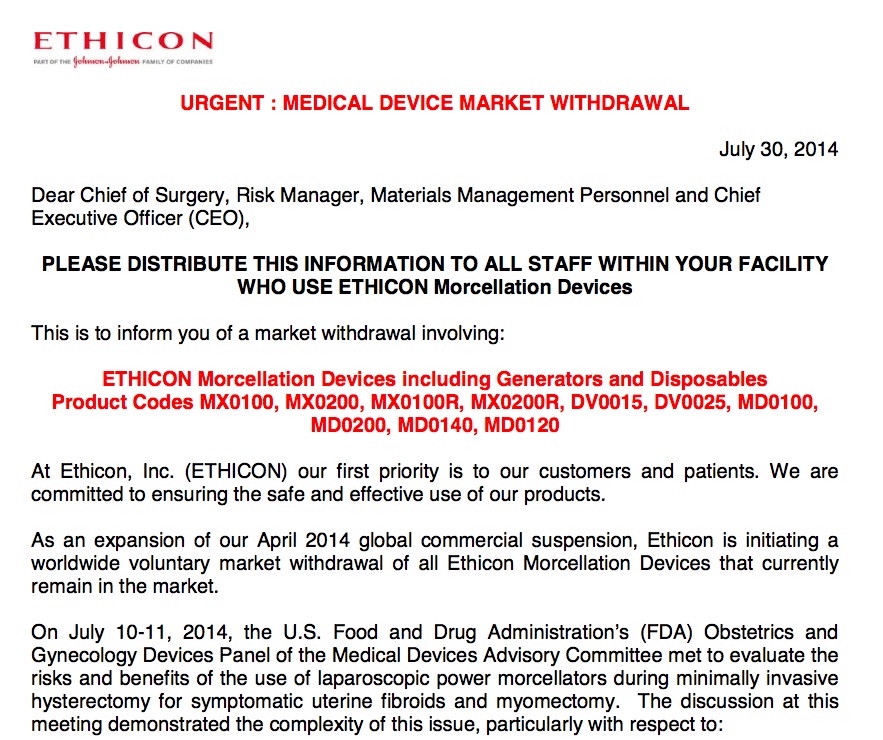 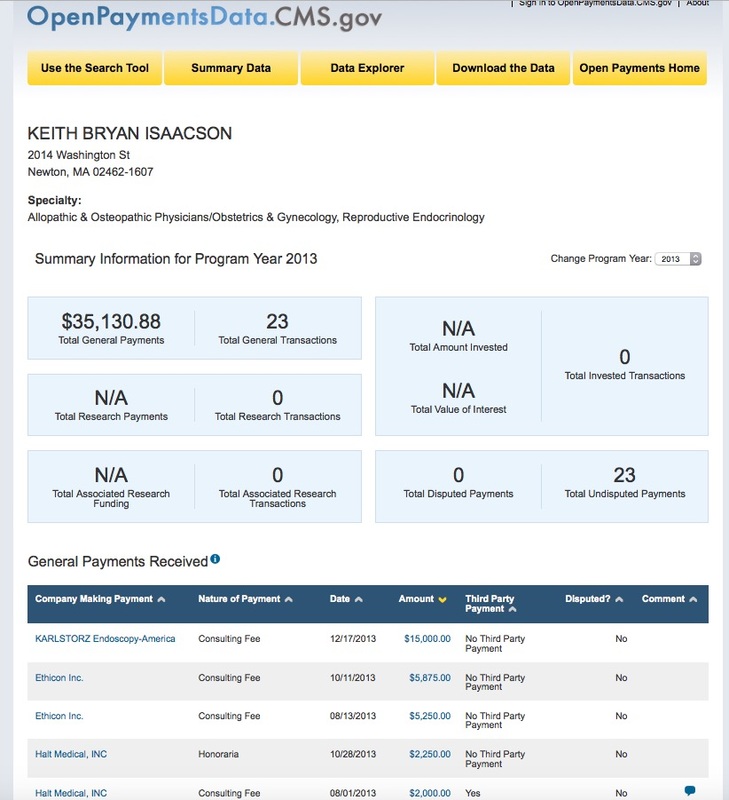 Dr. Javier Magrina of the Mayo Clinic was less enthusiastic. He'll do the surgery, but only using an endobag. He was also paid less by morcellation manufacturers. 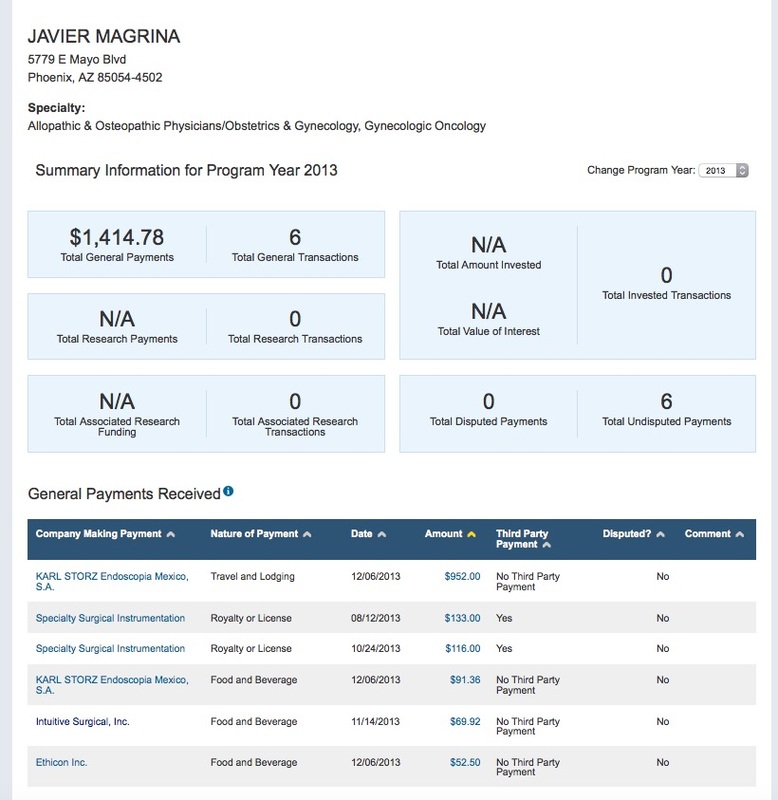 Read more at Drs. Reed and Noorchashm's page, here.
It appears that the trending press release, er, news story this week concerns the use of SSRI anti-depressants in pregnant women. The article, barely rewritten by health journalists at all the leading papers, says some risks are increased, others decreased. 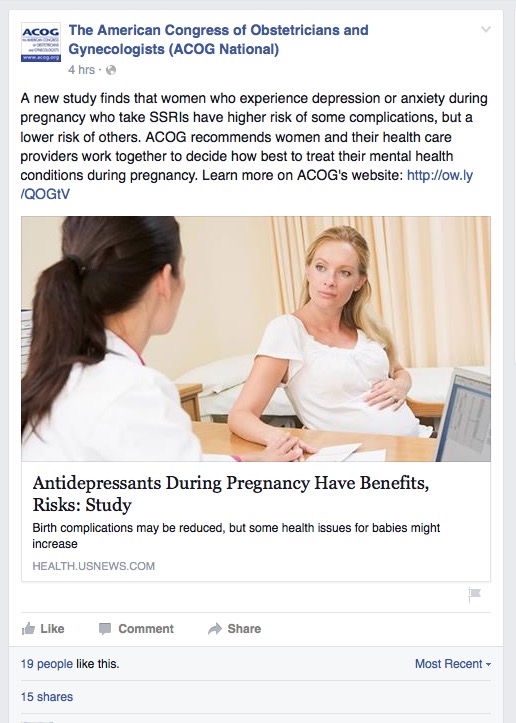 First question, always, when reading about a "new study" is, who paid for this? This one is based on an NIH and a Finnish grant, so the question of big pharma influence is a bit opaque, but because this one has been released in all the major publications at the same time, see picture at left, that's a good tip-off that pharma has a hand in there somewhere. Normally-financed studies that aren't reporting a major breakthrough don't get this kind of wide release.  The headline in the ACOG's Facebook post says, "ACOG recommends women and their health care providers work together..." This is something I have only seen the ACOG do. They suggest something to patients that may, in fact, not be beneficial at all, but if their suggestion of it to patients increases patients' likelihood to bring it up with their OBGYNs, well, that's just their choice. It's not readily obvious, but the ACOG is actually using the language they learned when talking about pro-choice issues. How many of us will read past that headline? According to a 2014 survey by the American Press Institute, only 4 in 10 of us will click through and read the article. http://www.americanpressinstitute.org/publications/reports/survey-research/rational-attentive-news-consumer/  So, what would the ACOG's readership miss if they're among the 59% who don't click on this article? Let's join the 41% and find out. The article, itself, is hard to get to. It's not the link within the copy above the picture. You have to click on the copy under the photo to get to it. Here's the study. “Our findings provide evidence that taking these antidepressants is associated with a lower risk of preterm birth and Caesarean section and further confirm the results from previous research of a higher risk for several neonatal problems,” noted Brown. “Given these divergent findings, the decision whether to prescribe these medications during pregnancy should be individualized to the mother’s medical and psychiatric history.” Well, no. This is only true if this study were all the data available to us, but that's far from the case. Instead, it looks like the vast majority of data about women who take SSRIs indicates that they are increasing the risk of their babies being born with birth defects. I don't know too many pregnant women who would be comfortable with that risk. 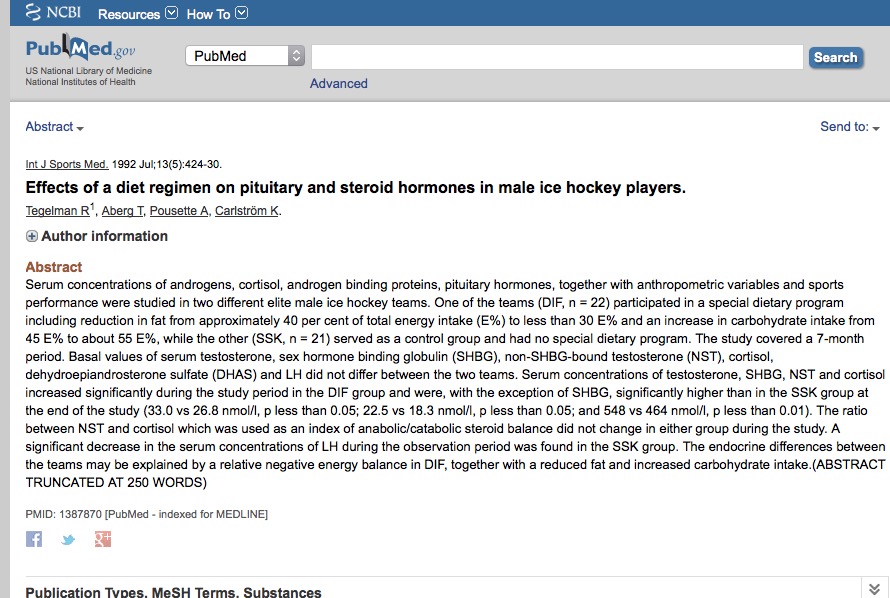 In fact, babies are born addicted to SSRIs, and with a host of birth defects. http://contemporaryobgyn.modernmedicine.com/contemporary-obgyn/content/tags/breastfeeding/use-selective-serotonin-reuptake-inhibitors-during-pre?page=full The study results are really very negative. "...women who took an SSRI during the second or third month of pregnancy had nearly twice the risk of having children with congenital malformations as women who took no SSRI during pregnancy" http://www.bmj.com/content/333/7573/824.5 In Finland, the study indicates that the percentage of pregnant women taking an SSRI is 4%. In the US? 10%. Are alternatives are tried first? Hormonal fluctuations can lead to depression, but is there a better, safer answer than SSRIs? Yes, of course. Even altering diet can have a beneficial effect. Wouldn't that be a better place to start? These are, after all, steroid hormones made by the ovaries that we're talking about, and the ovaries do link to the brain (the hypothalamus and pituitary) via the HPG axis. Can those steroid hormone levels be influenced by diet? Yes.  So, what about the information the ACOG links to on its own site through that little link in the copy above the picture? At the ACOG's own site, linked to from the article, we learn: 1) The tiny print along the top indicates that the content on the page is not about the study, but an advertisement. See the tiny print at the top, there? That's pretty important. 2) There's no indication of who paid for the ad. That doesn't stop people from taking it all at face value. But, wait, why is the ACOG advertising on its site at all? Isn't this a professional organization's site with unbiased information for patients and medical professionals? Nope. Far from it. Though I can't find any other physician organizations selling themselves in this way on their site, the ACOG has all kinds of ways you can pay to play. If I click on that little word "Advertisement" at the top of the Depression ad page, I'm brought here: http://www.acog.org/About_ACOG/Advertising.aspx 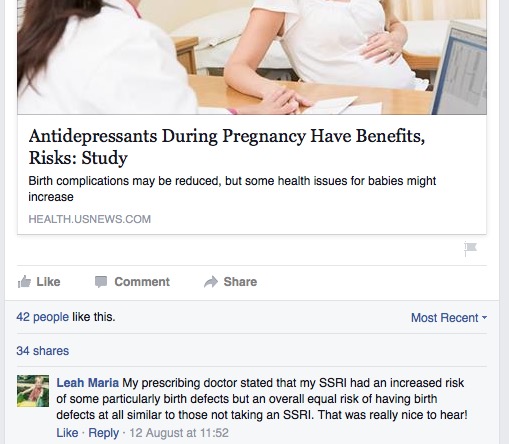  And if I click on the first link, Annual Meeting, and then Rate Card.pdf, I'm brought here. http://www.acog.org/-/media/Departments/Annual-Clinical-Meeting/acog2015ratecard.pdf?la=en  Holy crap. Even I am shocked.  That's all I have for today because I am speechless. Would you be surprised if you found out that you had no idea what menopause is? It sounds like a boring topic, and you suspect you already know, but what if you don't? I'll survey you at the end to see if this came as news to you. Meno: Bleeding Pause: End That's all that word means. Let's be very, very clear about this, because it leads to some uninformed and crucially poor choices on our part as women. It does NOT mean that your ovaries shrivel up and die. Not an illness The idea that menopause is an illness started in the 1940s when Wyeth Pharma, now part of Pfizer, started selling pills made from pregnant horse pee (yes, Premarin/PremPro really is derived from horse pee from horses kept in HORRIBLE conditions) to women for menopausal symptoms.
Menopause can suck, so if you want to use drugs, go for it. Just not Premarin or PremPro, please. Besides the inhumane conditions the horses are kept in, the drugs are also bad for your liver because you take them orally. PremPro is linked to breast cancer, and both are linked to stroke. Doctors who say they're not risky, or that the risks have been misconstrued because the WHI study was flawed, either do not understand it or are paid to prescribe them. It's another story, and I'll cover that another day. There are so many other, less risky choices. Whatever you might choose to take - know the risks. They all carry risks. But, bottom line: menopause is not an illness. It's just the natural course of things for every woman. By definition, that means it's the norm, not something that requires medication.
Some women have shared with me that their OBGYNs told them that their ovaries shrivel up to useless raisins that they may as well just remove. I won't use the harsh words I want to about that because this is about facts, not editorializing, so here are facts: 1. Menopause usually takes about 4-5 years and ends around age 51 for most women. 2. The hormones produced by the ovaries (no, not just estrogen, but estrogen, progesterone, testosterone, androstenedione, DHEA, and the proteins activin and inhibin) fluctuate. In some cases they fluctuate wildly, so some of us have more severe symptoms, like hot flashes and mood changes, than others. 3. When our endocrine system's chemistry is out of whack, it naturally affects the whole system. That system includes chemistry that is linked to depression, insomnia, anxiety, and ability to deal with stress - these chemicals are norepinephrine, dopamine, serotonin, and oxytocin. Unless you have things going on in your life - divorce, loss of a loved one, unemployment - that can explain your depression as psychological, understanding the effect of changing hormones on your body is essential to ensuring that you don't think it's "you" when it's not. These are BIOCHEMICAL reactions to the fact that your ovarian hormone levels are in flux as the ovaries are changing their function. It's a SYSTEM that works together, and big changes lead to big ripples. 4. Understanding your endocrine system at even the most basic level will help you to think about your body differently. It's not new age or 'one theory about the body' - it's hard science that makes the interconnectedness of things much clearer.
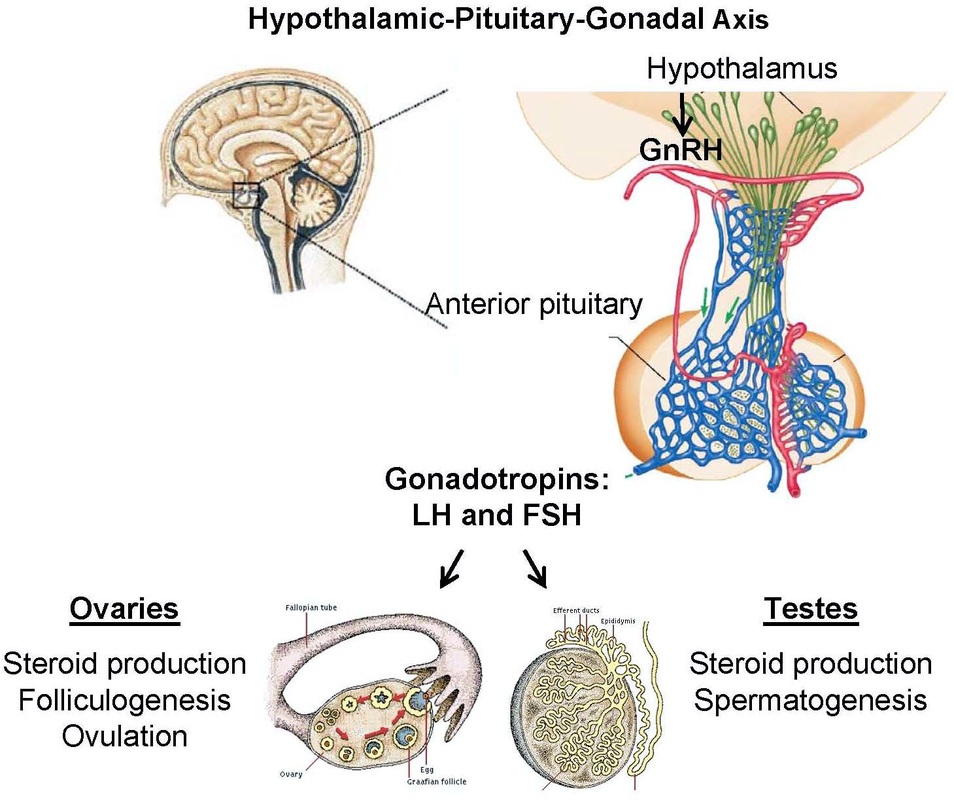
5. Testes and ovaries are both called gonads in medicine, and serve the two functions, shown above on the right. Women: ovulating, men: making sperm, and both: creating steroid hormones. 6. As with post-partum depression, rather than checking hormone levels and balancing them, many doctors instead put women on SSRI anti-depressants. (If you look at my link, above, imagine risking cardiac birth defects before trying to balance ovarian hormone levels?? See the tiny print at the top of the ACOG's page on that link that says that's an ad? What business do they have serving up ads for things linked to birth defects on that site?) 7. Women are already taking just a buttload of anti-depressants: According to the Centers for Disease Control & Prevention, U.S. women between the ages of 45 and 64 are on anti-depressants at a rate twice the national average. SSRI anti-depressants (SSRI = selective serotonin reuptake inhibitors, changing the way your brain handles one of those chemicals), like Prozac, may have their place when people are severely depressed, but it's my opinion that they're a life raft, not a boat. (So much for not editorializing.) These drugs can mask the problem by flattening or numbing us out, and in many cases make women feel like everything has been done that could be, so if they're not feeling better, it's up to them to work it out. I compare this to putting so many boys on ADD medication - flattening out the spikes in mood in both genders at either end of the age spectrum. Those moods may lead to problems in social settings or in terms of how we feel about ourselves, but is one blanket medication the right answer? Not if it doesn't get at the underlying cause. Not if it's just a pat on the head or done to make you easier for others to be around. That's not your job. When you're crashing, you put the oxygen mask on yourself before you try to help others. Your job is to get yourself well, not to hide your discomfort. Bottom line? In many cases, especially at times when hormones are in flux, it's not you, it's chemistry. 8. Whether the World Health Organization chooses to recognize it or not, men absolutely do experience an equivalent, andropause, as they age. Their hormone levels, including testosterone, do decline, but that change doesn't result in the same side effects, so it doesn't receive the same attention. If the same chemical changes were taking place in men, they'd be feeling and acting the same way we women do, so do NOT beat yourself up. DO advocate for yourself. We've tolerated cycling monthly hormones in order to produce ALL the world's people - we deserve better than the use of the pejorative "hormonal." And we do not deserve to be treated as though everything we experience is psychological or psychosomatic when it's quite clear that it's very often biochemistry.  8. But I promised you that something about this was wonderful. I'm going to deliver on that promise now. When menopause is done, something has happened that is pretty damned magical. It's one of life's absolutely beautiful and miraculous changes - no exaggeration. The ovaries do shrink down when women get to about age 50, but not to turn into useless raisins. That's NOT who we are once we're done being able to reproduce. Turns out that there's more to us than just making babies. We are meant to live long, full lives. 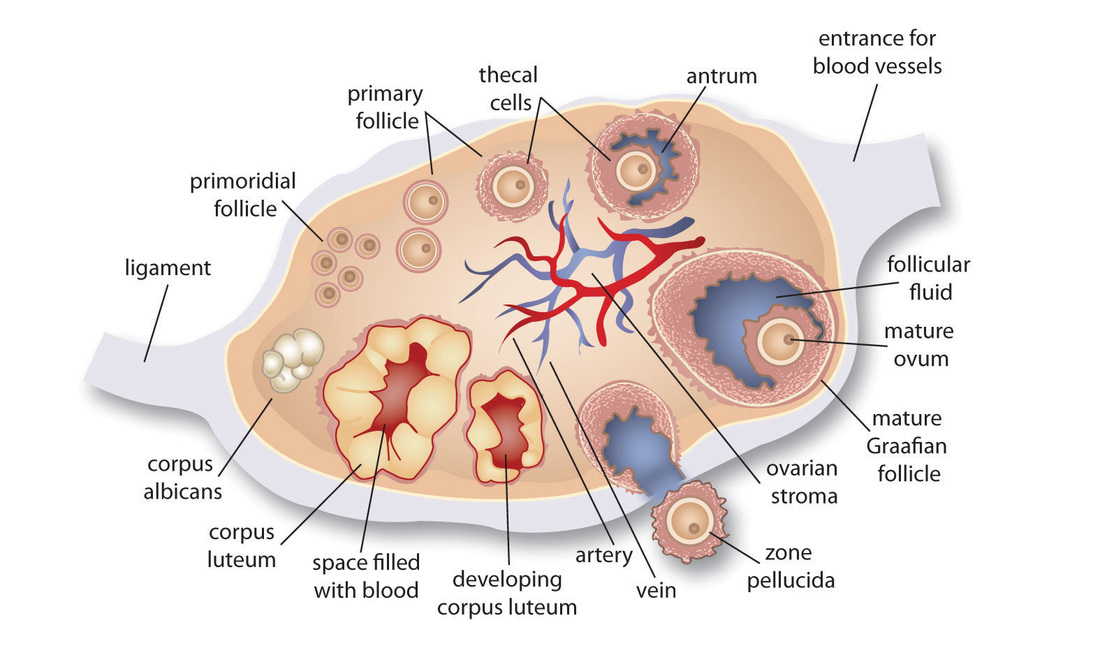 The ovaries' stroma begins to emit a different mix of hormones. We had always made androgens - testosterone, androstenedione, and their precursor, DHEA. Now, we make more than we did before, and in an amount that increases throughout our 60s and levels off in our 70s. Yes, this brings many of us those awesome chin hairs. It's true. That is NOT damned magical, but along with this, this change in what our ovaries produce makes muscle mass, balanced brain chemistry, our bones stronger, and our hearts stronger - all kinds of things...and that is why I think of this as the changing of the guard. We don't need the outside for all the egg producing tasks, but we do need the inside for the hormones it makes, so that becomes the focus. Our bodies are so smart! Our ovaries are just adapting to our changing needs. Isn't that kind of amazing? Why isn't it taught? I don't know... Instead, we're taught they're part of the "reproductive system," and while that's true, it's misleading. So, yes, menopause symptoms can suck, but it's the price we pay to allow our ovaries to turn into machines that protect our health, mood, and strength as we age. |

Ovaries for Life
Archives
October 2015
Categories |




 RSS Feed
RSS Feed
