I made a little movie to help make it clear.
|
The CDC used to publish what they referred to as a surveillance of hysterectomy in the U.S. every 5 or so years. Since 2005, they've stopped, or at least stopped publishing them online, and have even taken down the 2000-2004 report.
Apart from surveys that are done only very infrequently, the last one being in 1996, the CDC has only ever published the number of inpatient hysterectomies. This is the basis for the number we see cited so commonly in studies and literature, 600,000. However, this is increasingly inaccurate as the level of outpatient, or ambulatory, hysterectomies rises. A well-corroborated number from the AHRQ indicates that at least 40%-50% of all hysterectomies are now done on an outpatient basis. This doesn't mean that the patient goes home the same day. An outpatient patient can actually end up spending several nights in the hospital but the doctor never admits her. Her insurance likes this because they pay less for an outpatient procedure. Anyhow, if we use the 40% figure, we know that the last-reported CDC inpatient number was 498,000. That means that, if inpatient is 60%, that's about a 830,000 total of U.S. hysterectomies. To arrive at the number of elective hysterectomies, let's be really conservative and take out every woman diagnosed with uterine (55,000), ovarian (22,000), and cervical (13,000) cancer, based on SEER stats (e.g., http://seer.cancer.gov/statfacts/html/cervix.html). That leaves 740,000 elective (voluntary) hysterectomies. If we stick with the accepted "55% of elective hysterectomies include bilateral ovary removals" estimate, that's about 407,000 women a year whose ovaries are removed during elective hysterectomy. However, the number of healthy ovary removals may increase to ~700,000 a year if Dr. Rocca is right in his write-up that there are 300,000 additional BSOs when women present with benign cysts. Potentially, we are talking about ~1,900 women a day to remove an organ that only develops cancer in 22,000 women a year. But are all these random ovary removals the reason the number is so low? No. The ovarian cancer diagnosis and mortality rate was the same in 1965 when the ovarian removal rate was only 25%. With such a low risk, removing the ovaries of a woman at risk is like shooting fish in a barrel. Taking out hundreds of thousands to address the risk in ~20,000 is like using a boulder to crush an ant. It's also not a surgical approach taken in any other cancer prevention surgery. The ACOG argues that this should ultimately be up to the woman. Unless the woman does not have a demonstrated (via a certified genetic counselor) risk of ovarian cancer, this is not true. Once the doctor says "cancer risk" to the patient, she will agree to anything. If they couple that with their 2011 brochure that says that the ovaries cease functioning at the time of menopause, which we've known for 100 years since the endocrine system because well-understood is not true, then you are setting up enough misinformation for us to stay where we are: hundreds of thousands of women made ill to address a microscopic risk. This is NOT about informed consent, but about bad medicine. The statistics are staggering. Why women without ovaries are more likely to develop Alzheimer's and other dementia; Parkinson's; and lung cancer - a hypothesis. Also, why calcium supplements are not the answer to our increased risk of death by fracture.
 Researchers increasingly tie high LDL (low density lipid, a.k.a., bad) cholesterol to the Lewy bodies/plaque that they see in these patients. They see the high cholesterol affect patients who've had some kind of heart or TBI (traumatic brain injury) issue, but I'd guess that not being able to regenerate normally because activin is absent could have the same result. Without a response from the ovaries to the luteinizing hormone (LH) sent to them by the pituitary gland, the luteinizing hormone levels just keep going up, unchecked. Higher levels of luteinizing hormone are also tied to Alzheimer's in women, so the risk profile of women without ovaries becomes more complex but the fact that she has increased risk becomes clearer. (LH/Alzheimer's study here: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2111407/ - though the study author is incorrect, of course, when she says that postmenopausal women have lost their ability to produce estrogen. This is not true of either BSO women or naturally postmenopausal women, but is more true of BSO women. At a minimum, the adrenal glands contribute androgens that convert to estrogen. In women who keep their ovaries, their testosterone rises after menopause and some of it converts to estrogen, leading to higher levels in postmenopausal women than BSO women.)  My thinking is that it is the missing activin, a cytokine protein produced by the gonads (ovaries), at play when there are issues with the lungs (also the arteries, due to activin's role in elasticity and smooth muscle). Lung alveoli rely on activin. This may be why I read about (and have personally experienced) asthma as one of the first health issues in BSO women, and may also be the reason that regeneration issues and lack of activin (cytokine) activity to reduce inflammation lead to lung cancer and other lung issues, even in women who haven't smoked. We know that using hormones, as many women without ovaries do, increases this risk even further, to 2.4x. 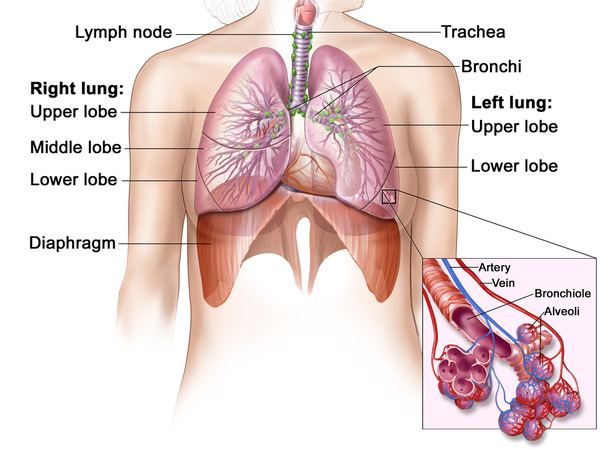 The significantly lower testosterone they find in women without ovaries, in, for example, the Fogle and Rancho Bernardo studies, is one aspect of heart and other muscular weakness, but activin is likely a separate contributory factor.
Finally, this week's article in the New England Journal of Medicine about the fact that calcium supplements weren't show to reduce fracture is not surprising. Fracture is not so much about bone mineral strength but about bone's flexibility that comes from the net made by collagen. The lack of flexibility that comes with the decline in collagen in bone is likely the underlying issue with fracture in women without ovaries, not the lack of calcium in her diet. Our bones are more brittle for the same reason that our skin is dry and lifeless. It's also the reason so many of us experience painful osteoarthritis and fibromyalgia - lack of collagen in joints. Activin is too often overlooked, and contributes to a host of health issues of its own. I keep coming back to it as our biggest blind spot with women who've had a BSO. Alzheimer's costs the U.S. $2 billion a year right now, and that number is projected to increase 5x by 2050. Maybe we could check some of that if we stopped removing healthy ovaries 1,900 times a day in this country. For more information, visit www.overy.org or email at [email protected]. |

Ovaries for Life
Archives
October 2015
Categories |

 RSS Feed
RSS Feed
