Would you be surprised if you found out that you had no idea what menopause is? It sounds like a boring topic, and you suspect you already know, but what if you don't?
I'll survey you at the end to see if this came as news to you.
Meno: Bleeding
Pause: End
That's all that word means. Let's be very, very clear about this, because it leads to some uninformed and crucially poor choices on our part as women. It does NOT mean that your ovaries shrivel up and die.
Not an illness
The idea that menopause is an illness started in the 1940s when Wyeth Pharma, now part of Pfizer, started selling pills made from pregnant horse pee (yes, Premarin/PremPro really is derived from horse pee from horses kept in HORRIBLE conditions) to women for menopausal symptoms.
I'll survey you at the end to see if this came as news to you.
Meno: Bleeding
Pause: End
That's all that word means. Let's be very, very clear about this, because it leads to some uninformed and crucially poor choices on our part as women. It does NOT mean that your ovaries shrivel up and die.
Not an illness
The idea that menopause is an illness started in the 1940s when Wyeth Pharma, now part of Pfizer, started selling pills made from pregnant horse pee (yes, Premarin/PremPro really is derived from horse pee from horses kept in HORRIBLE conditions) to women for menopausal symptoms.
 1950s Premarin ads |  Nice, huh? |
Menopause can suck, so if you want to use drugs, go for it. Just not Premarin or PremPro, please. Besides the inhumane conditions the horses are kept in, the drugs are also bad for your liver because you take them orally. PremPro is linked to breast cancer, and both are linked to stroke. Doctors who say they're not risky, or that the risks have been misconstrued because the WHI study was flawed, either do not understand it or are paid to prescribe them. It's another story, and I'll cover that another day. There are so many other, less risky choices. Whatever you might choose to take - know the risks. They all carry risks.
But, bottom line: menopause is not an illness. It's just the natural course of things for every woman. By definition, that means it's the norm, not something that requires medication.
 | Changing of the guard |
Some women have shared with me that their OBGYNs told them that their ovaries shrivel up to useless raisins that they may as well just remove. I won't use the harsh words I want to about that because this is about facts, not editorializing, so here are facts:
1. Menopause usually takes about 4-5 years and ends around age 51 for most women.
2. The hormones produced by the ovaries (no, not just estrogen, but estrogen, progesterone, testosterone, androstenedione, DHEA, and the proteins activin and inhibin) fluctuate. In some cases they fluctuate wildly, so some of us have more severe symptoms, like hot flashes and mood changes, than others.
3. When our endocrine system's chemistry is out of whack, it naturally affects the whole system. That system includes chemistry that is linked to depression, insomnia, anxiety, and ability to deal with stress - these chemicals are norepinephrine, dopamine, serotonin, and oxytocin. Unless you have things going on in your life - divorce, loss of a loved one, unemployment - that can explain your depression as psychological, understanding the effect of changing hormones on your body is essential to ensuring that you don't think it's "you" when it's not.
These are BIOCHEMICAL reactions to the fact that your ovarian hormone levels are in flux as the ovaries are changing their function. It's a SYSTEM that works together, and big changes lead to big ripples.
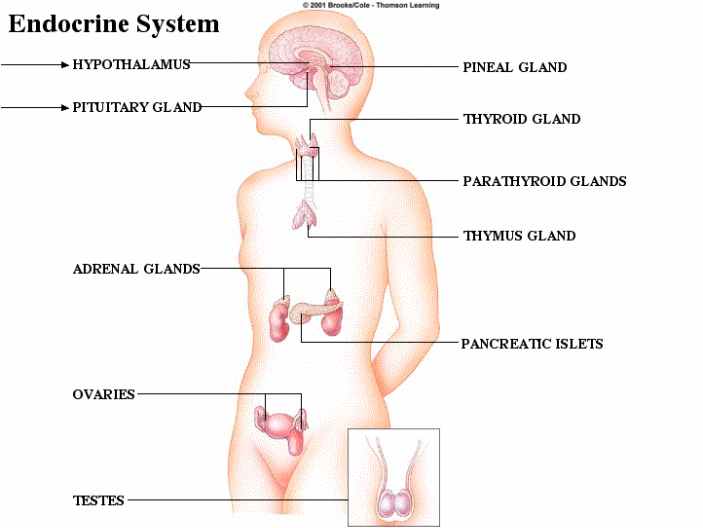
4. Understanding your endocrine system at even the most basic level will help you to think about your body differently. It's not new age or 'one theory about the body' - it's hard science that makes the interconnectedness of things much clearer.
1. Menopause usually takes about 4-5 years and ends around age 51 for most women.
2. The hormones produced by the ovaries (no, not just estrogen, but estrogen, progesterone, testosterone, androstenedione, DHEA, and the proteins activin and inhibin) fluctuate. In some cases they fluctuate wildly, so some of us have more severe symptoms, like hot flashes and mood changes, than others.
3. When our endocrine system's chemistry is out of whack, it naturally affects the whole system. That system includes chemistry that is linked to depression, insomnia, anxiety, and ability to deal with stress - these chemicals are norepinephrine, dopamine, serotonin, and oxytocin. Unless you have things going on in your life - divorce, loss of a loved one, unemployment - that can explain your depression as psychological, understanding the effect of changing hormones on your body is essential to ensuring that you don't think it's "you" when it's not.
These are BIOCHEMICAL reactions to the fact that your ovarian hormone levels are in flux as the ovaries are changing their function. It's a SYSTEM that works together, and big changes lead to big ripples.
4. Understanding your endocrine system at even the most basic level will help you to think about your body differently. It's not new age or 'one theory about the body' - it's hard science that makes the interconnectedness of things much clearer.
 | 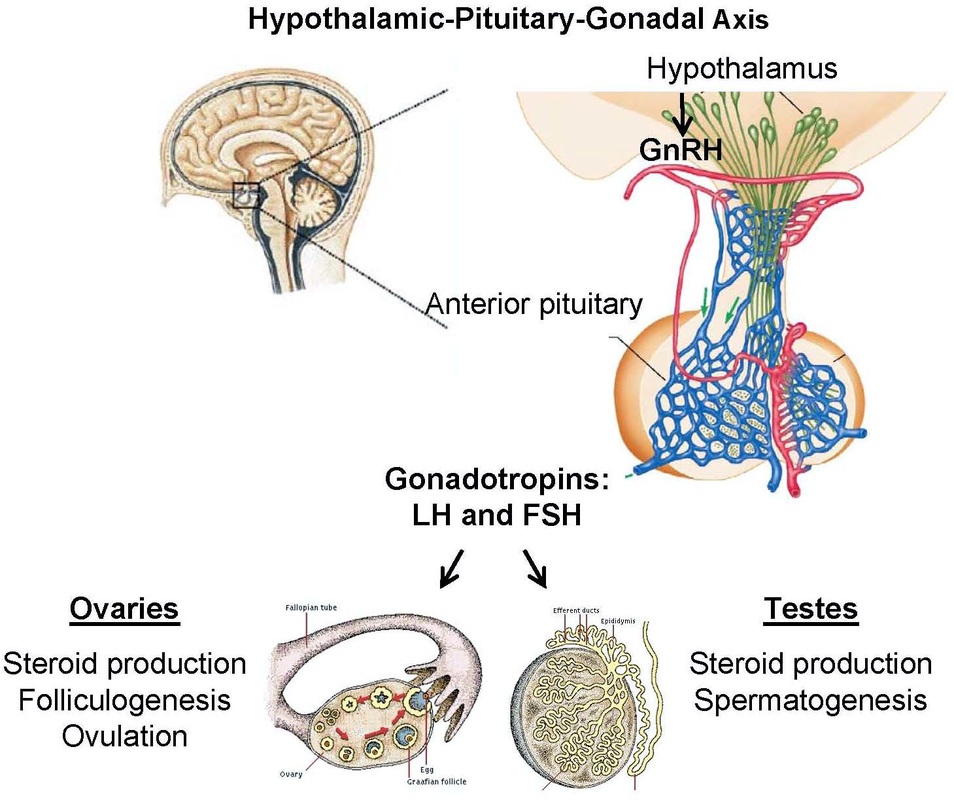 |
5. Testes and ovaries are both called gonads in medicine, and serve the two functions, shown above on the right. Women: ovulating, men: making sperm, and both: creating steroid hormones.
6. As with post-partum depression, rather than checking hormone levels and balancing them, many doctors instead put women on SSRI anti-depressants.
(If you look at my link, above, imagine risking cardiac birth defects before trying to balance ovarian hormone levels?? See the tiny print at the top of the ACOG's page on that link that says that's an ad? What business do they have serving up ads for things linked to birth defects on that site?)
7. Women are already taking just a buttload of anti-depressants: According to the Centers for Disease Control & Prevention, U.S. women between the ages of 45 and 64 are on anti-depressants at a rate twice the national average. SSRI anti-depressants (SSRI = selective serotonin reuptake inhibitors, changing the way your brain handles one of those chemicals), like Prozac, may have their place when people are severely depressed, but it's my opinion that they're a life raft, not a boat. (So much for not editorializing.)
These drugs can mask the problem by flattening or numbing us out, and in many cases make women feel like everything has been done that could be, so if they're not feeling better, it's up to them to work it out.
I compare this to putting so many boys on ADD medication - flattening out the spikes in mood in both genders at either end of the age spectrum. Those moods may lead to problems in social settings or in terms of how we feel about ourselves, but is one blanket medication the right answer? Not if it doesn't get at the underlying cause. Not if it's just a pat on the head or done to make you easier for others to be around. That's not your job. When you're crashing, you put the oxygen mask on yourself before you try to help others. Your job is to get yourself well, not to hide your discomfort.
Bottom line? In many cases, especially at times when hormones are in flux, it's not you, it's chemistry.
8. Whether the World Health Organization chooses to recognize it or not, men absolutely do experience an equivalent, andropause, as they age. Their hormone levels, including testosterone, do decline, but that change doesn't result in the same side effects, so it doesn't receive the same attention.
If the same chemical changes were taking place in men, they'd be feeling and acting the same way we women do, so do NOT beat yourself up. DO advocate for yourself. We've tolerated cycling monthly hormones in order to produce ALL the world's people - we deserve better than the use of the pejorative "hormonal." And we do not deserve to be treated as though everything we experience is psychological or psychosomatic when it's quite clear that it's very often biochemistry.
(If you look at my link, above, imagine risking cardiac birth defects before trying to balance ovarian hormone levels?? See the tiny print at the top of the ACOG's page on that link that says that's an ad? What business do they have serving up ads for things linked to birth defects on that site?)
7. Women are already taking just a buttload of anti-depressants: According to the Centers for Disease Control & Prevention, U.S. women between the ages of 45 and 64 are on anti-depressants at a rate twice the national average. SSRI anti-depressants (SSRI = selective serotonin reuptake inhibitors, changing the way your brain handles one of those chemicals), like Prozac, may have their place when people are severely depressed, but it's my opinion that they're a life raft, not a boat. (So much for not editorializing.)
These drugs can mask the problem by flattening or numbing us out, and in many cases make women feel like everything has been done that could be, so if they're not feeling better, it's up to them to work it out.
I compare this to putting so many boys on ADD medication - flattening out the spikes in mood in both genders at either end of the age spectrum. Those moods may lead to problems in social settings or in terms of how we feel about ourselves, but is one blanket medication the right answer? Not if it doesn't get at the underlying cause. Not if it's just a pat on the head or done to make you easier for others to be around. That's not your job. When you're crashing, you put the oxygen mask on yourself before you try to help others. Your job is to get yourself well, not to hide your discomfort.
Bottom line? In many cases, especially at times when hormones are in flux, it's not you, it's chemistry.
8. Whether the World Health Organization chooses to recognize it or not, men absolutely do experience an equivalent, andropause, as they age. Their hormone levels, including testosterone, do decline, but that change doesn't result in the same side effects, so it doesn't receive the same attention.
If the same chemical changes were taking place in men, they'd be feeling and acting the same way we women do, so do NOT beat yourself up. DO advocate for yourself. We've tolerated cycling monthly hormones in order to produce ALL the world's people - we deserve better than the use of the pejorative "hormonal." And we do not deserve to be treated as though everything we experience is psychological or psychosomatic when it's quite clear that it's very often biochemistry.
8. But I promised you that something about this was wonderful. I'm going to deliver on that promise now. When menopause is done, something has happened that is pretty damned magical. It's one of life's absolutely beautiful and miraculous changes - no exaggeration.
The ovaries do shrink down when women get to about age 50, but not to turn into useless raisins. That's NOT who we are once we're done being able to reproduce. Turns out that there's more to us than just making babies. We are meant to live long, full lives.
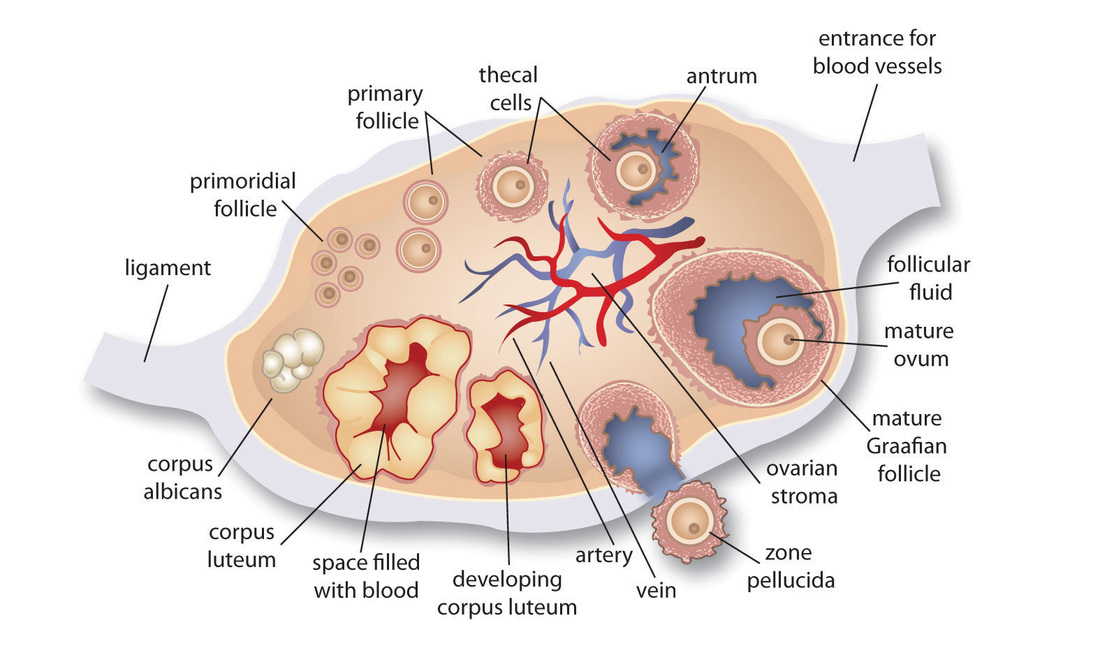
The ovaries' stroma begins to emit a different mix of hormones. We had always made androgens - testosterone, androstenedione, and their precursor, DHEA. Now, we make more than we did before, and in an amount that increases throughout our 60s and levels off in our 70s.
Yes, this brings many of us those awesome chin hairs. It's true. That is NOT damned magical, but along with this, this change in what our ovaries produce makes muscle mass, balanced brain chemistry, our bones stronger, and our hearts stronger - all kinds of things...and that is why I think of this as the changing of the guard. We don't need the outside for all the egg producing tasks, but we do need the inside for the hormones it makes, so that becomes the focus.
Our bodies are so smart! Our ovaries are just adapting to our changing needs. Isn't that kind of amazing? Why isn't it taught? I don't know... Instead, we're taught they're part of the "reproductive system," and while that's true, it's misleading. So, yes, menopause symptoms can suck, but it's the price we pay to allow our ovaries to turn into machines that protect our health, mood, and strength as we age.

 RSS Feed
RSS Feed
